Negative Controls: The Bias Check Most Observational Studies Skip
📖 15 min read · Published Apr 10, 2026
Most observational studies spend pages adjusting for confounding, then act shocked when reviewers ask whether residual bias is still driving the result. That is exactly what they should ask. A negative control is one of the cleanest ways to stress-test your design. If your treatment appears to cause an outcome it cannot plausibly cause, or your outcome appears to be caused by an exposure that happens too late or should be irrelevant, your main estimate is probably contaminated.
Negative controls do not magically fix bias. They do something more honest. They tell you whether your supposedly careful design is still leaking confounding, selection problems, or measurement artifacts. In other words, they are not a decorative sensitivity analysis. They are a credibility check.
The Core Idea
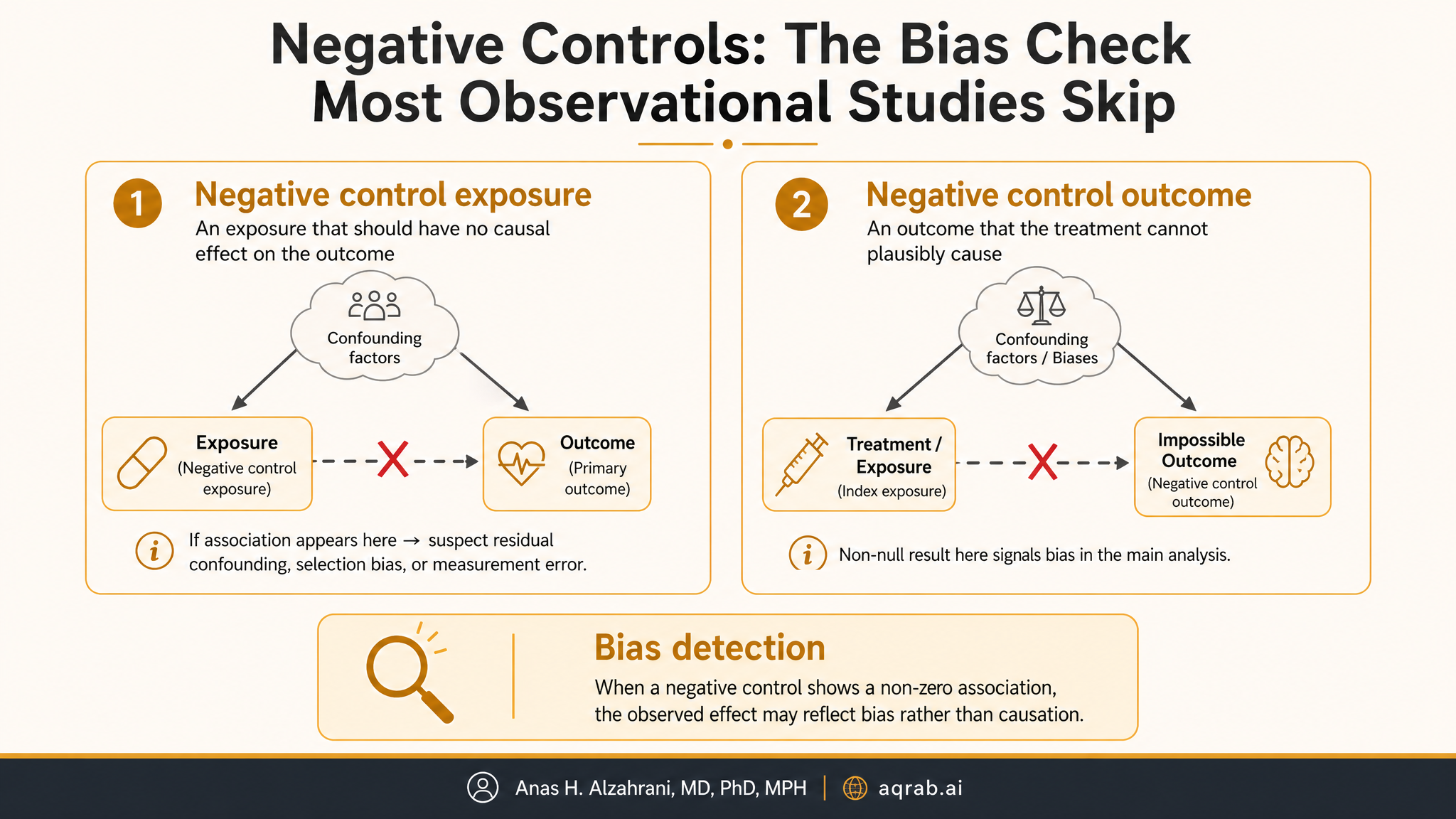
A negative control is a variable chosen specifically because it should not have the causal relationship your main analysis is claiming.
Negative control outcome
An outcome the exposure should not plausibly affect. If you still observe an association, that suggests residual bias.
Negative control exposure
An exposure that should not plausibly affect the outcome. If it does, your design is probably picking up confounding or selection rather than causation.
The logic is beautifully simple. If bias creates fake effects in the negative control analysis, that same bias may also be distorting your main estimate.
Clinical example:
Suppose you study whether statin initiation reduces dementia risk. A reasonable negative control outcome might be acute traumatic injury shortly after treatment initiation, assuming no plausible short-term causal pathway. If statin users also appear protected against trauma, you may be seeing healthy-user bias rather than a neuroprotective effect.
What Negative Controls Can Detect
Residual confounding
The most common use. If unmeasured patient differences create a fake effect in the negative control, they may be driving your main association too.
Selection bias
Conditioning on who gets measured, treated, or retained can induce associations even when no causal path exists.
Measurement bias
Differential surveillance, coding intensity, or healthcare contact can create spurious relationships across outcomes that share the same detection system.
Temporal design mistakes
Future exposures predicting past outcomes, or implausibly immediate treatment effects, are often signs that time zero is broken.
What negative controls cannot do is prove the absence of bias. Passing a negative control is reassuring, but it does not certify the main analysis as causal truth. It only says the particular bias pattern you tested was not obvious in that diagnostic.
A Negative Control Is Not Just “Any Unrelated Variable”
This is where people get sloppy. A good negative control must be chosen for a causal reason, not because it feels random. You need a clear argument that:
- the exposure should not affect the negative control outcome, or
- the negative control exposure should not affect the outcome, and
- the negative control shares the same important bias structure as the main analysis.
That last part matters. If the negative control does not travel through the same confounding or measurement channels, then a null result is nearly meaningless. You tested the wrong leak.
Rule of thumb:
The best negative control feels boringly similar to the main analysis, except for the one thing that matters: the causal effect should be absent.
Negative Control Outcomes vs Exposures
| Type | Best use | Common example |
|---|---|---|
| Negative control outcome | When you suspect exposure groups differ in latent health-seeking behavior, frailty, or surveillance | Drug exposure predicting an implausibly unrelated injury or diagnosis |
| Negative control exposure | When you suspect the exposure measurement process itself is confounded | Future treatment assignment or a biologically irrelevant comparator exposure |
In pharmacoepidemiology, negative control outcomes are especially useful because healthy-user bias, contraindication bias, and differential healthcare contact love to masquerade as treatment effects. In policy studies, negative control exposures can reveal misaligned timing or hidden regional differences that the main model failed to absorb.
Design Example: Vaccine Uptake and Hospitalization
Imagine you are estimating whether influenza vaccination reduces all-cause winter hospitalization in older adults using claims data. Even with rich covariate adjustment, vaccinated patients may differ from unvaccinated patients in health behavior, trust in clinicians, mobility, and baseline frailty.
A strong negative control outcome might be hospitalization for an event that should not plausibly be prevented by the vaccine in the short term, but is captured by the same claims system and affected by the same care-seeking patterns. If vaccination appears to reduce that outcome too, your main estimate is waving a giant confounding flag.
This does not mean the vaccine has no benefit. It means your observational design cannot cleanly separate vaccine effect from who chooses vaccination.
The DAG Logic
Negative controls make the most sense when you think in DAGs, not vibes. Ideally, the negative control shares the same backdoor paths as the main exposure-outcome pair but lacks the direct causal arrow you are claiming.
If unmeasured confounder U affects both treatment A and outcome Y, and also affects negative control outcome Ync, then an observed association between A and Ync suggests residual confounding through U. That is the whole game.
What you want conceptually:
- Main analysis: A → Y may exist, but A ← U → Y is also possible.
- Negative control: A should not cause Ync, but A ← U → Ync may still exist.
- If A associates with Ync, residual bias through U is still alive.
How to Analyze Negative Controls
The simplest version is often the right one: run the same design you used in the main analysis on the negative control. Same cohort logic, same covariates, same weighting or matching strategy, same time zero discipline if possible.
- Define the main causal estimand first.
- Choose a negative control that shares the relevant bias channels.
- Replicate the analytic pipeline on the negative control analysis.
- Interpret the negative control as a diagnostic, not as an isolated result.
If the negative control estimate is near null with tight uncertainty, great, that increases confidence. If it is clearly non-null, do not bury it in a supplement and pretend the main result survived. That is exactly the moment to reconsider the design.
What a Failed Negative Control Means
Hard truth:
A clearly failed negative control means your design is not as credible as your main abstract probably sounds.
It does not automatically tell you the size or direction of bias in the main estimate. Bias affecting the negative control may be stronger, weaker, or structurally different. But it does tell you the design still contains non-causal signal. That should change your language, your confidence, and maybe your willingness to make causal claims at all.
The right response is usually one of three things:
- tighten the design, for example by improving time zero, active comparators, or covariate measurement,
- downgrade causal interpretation and report the finding as associational, or
- use the failed negative control as evidence that residual bias remains and discuss it plainly.
Common Mistakes
❌ Picking a negative control with a hidden plausible effect
If the exposure might actually affect the negative control, your diagnostic collapses immediately.
❌ Changing the entire analytic pipeline
A negative control only tests the main design if you keep the design structure meaningfully parallel.
❌ Declaring victory because the confidence interval crosses the null
A noisy negative control tells you little. Precision matters.
❌ Treating a negative control like a magic correction
Some methods use negative controls to calibrate estimates, but that only works under additional assumptions. The diagnostic role comes first.
Negative Controls in Modern Causal Workflows
Negative controls pair well with other design diagnostics. They are especially useful alongside active comparator designs, target trial emulation, E-values, balance checks, and falsification endpoints. Together, these tools answer a more serious question than “is the p-value below 0.05?” They ask whether the study deserves belief.
In high-stakes clinical observational work, that is the right standard. If a finding changes practice, reimbursement, or public messaging, you should want every plausible opportunity to prove yourself wrong before publication.
What Reviewers Should Expect
- A clear justification for why the chosen negative control should be causally null.
- An explanation for how it shares the relevant bias structure with the main analysis.
- Use of a parallel analytic pipeline.
- Honest interpretation if the negative control is non-null.
- No spin, no burying, no “supportive but not central” nonsense when the result undercuts the main design.
Bottom Line
Negative controls are one of the best tools for exposing causal overconfidence in observational research. They do not rescue a weak design, but they can reveal when the design is lying to you. That alone makes them worth using.
If your study makes a serious causal claim and you skipped negative controls because they were inconvenient, I am going to assume you preferred a cleaner narrative over a harder truth. Reviewers should assume the same.