Interference & Spillover Effects: When One Patient's Treatment Changes Another's Outcome
A lot of causal inference teaching quietly assumes that one person's treatment affects only that person. That assumption is convenient, elegant, and often false. Vaccination changes transmission. Antibiotic stewardship changes prescribing norms. ICU staffing interventions affect the whole ward. Digital health nudges spread through families, clinics, and WhatsApp groups whether you like it or not. When one unit's treatment changes another unit's outcome, you have interference, and pretending otherwise does not make the bias disappear.
This is where a lot of otherwise solid studies get sloppy. They estimate an average treatment effect as if the world were sealed into little independent bubbles, then write a discussion section about possible spillovers like it is a side note. It is not a side note. If interference is real, the estimand changes. You are no longer asking only what happens when I get treated. You are asking what happens when others around me get treated too.
The Assumption That Breaks: SUTVA
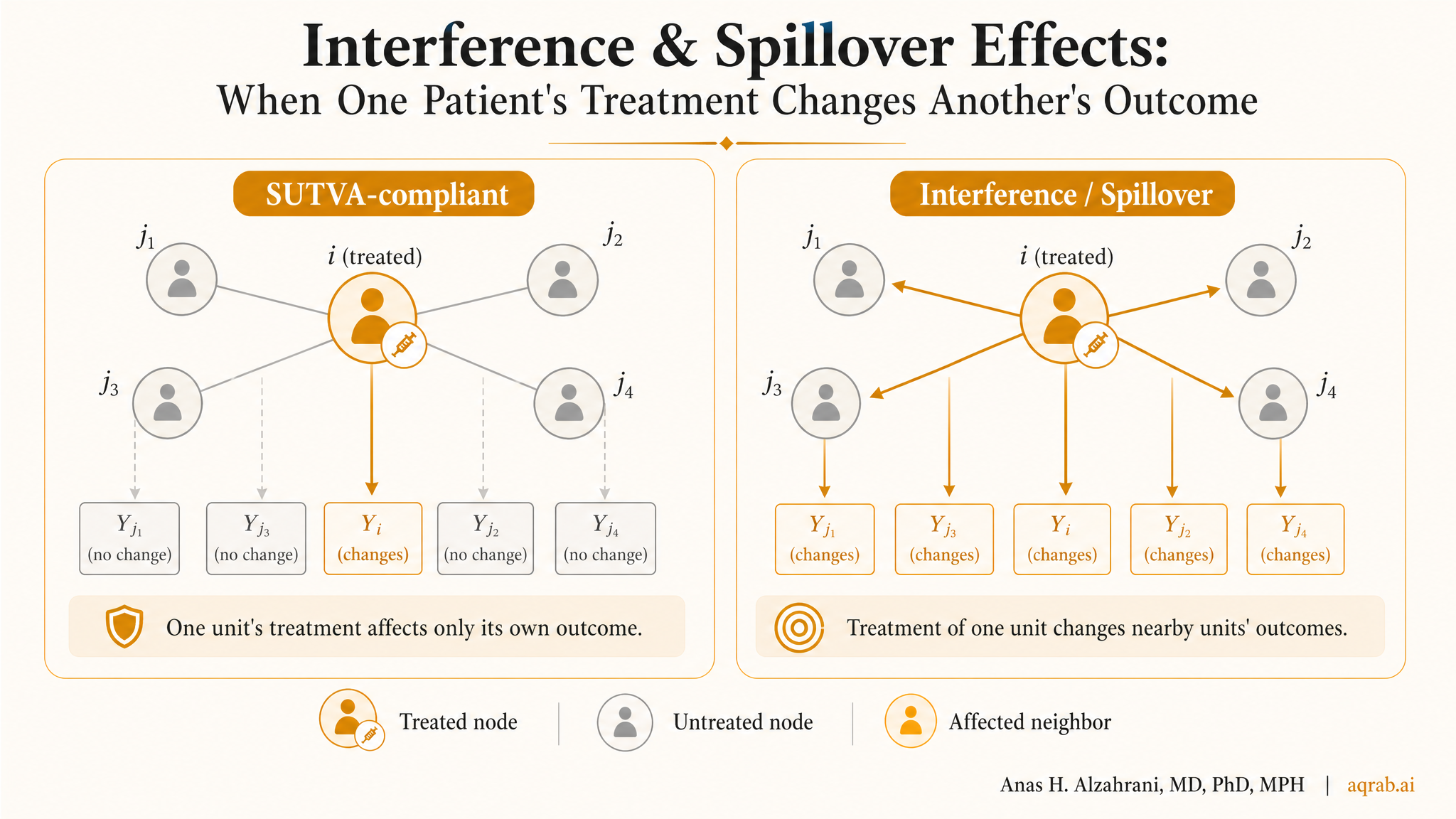
Most basic causal estimators rely on part of the Stable Unit Treatment Value Assumption, or SUTVA. One piece says there are no hidden versions of treatment. The other says there is no interferencebetween units. That second piece is the problem here.
When SUTVA fails:
Your outcome may depend not only on your own treatment but also on treatment coverage in your ward, clinic, household, village, or network. Standard individual-level treatment effect language stops being enough.
This does not mean causal inference is impossible. It means the lazy estimand is gone. You need to define the exposure mapping, the relevant group structure, and the effect you actually care about.
What Interference Looks Like in Real Research
Infectious disease
Vaccinating one person can reduce exposure risk for others. The indirect effect may be as important as the direct one.
Hospital policy
A handoff protocol or stewardship intervention changes team behavior, not just the patient officially enrolled.
Behavioral interventions
Smoking cessation, diet, and adherence spill across couples, families, peer groups, and clinicians.
Platform and policy studies
Interventions change information flow, waiting times, or referral patterns for everyone downstream.
Direct Effects Are No Longer the Whole Story
Once interference exists, one treatment can generate multiple causal effects. The cleanest conceptual split is:
- Direct effect: the effect of your own treatment, holding others' treatment fixed.
- Indirect or spillover effect: the effect of others being treated on your outcome, holding your own treatment fixed.
- Total effect: the combined effect of changing your treatment and the surrounding treatment pattern.
- Overall effect: the effect of shifting the treatment strategy for the entire group or cluster.
If a paper with obvious spillovers reports only “the treatment effect” without saying which of those it means, it is being imprecise at best and wrong at worst.
The First Real Design Choice: What Is the Relevant Group?
Interference almost never spreads randomly across the whole population. It usually follows a structure: household, ward, school, village, physician panel, social network, geographic catchment, or referral chain. Your job is to define the plausible boundary of spillover.
That boundary is not just technical window dressing. It determines who can affect whom, what exposure summaries make sense, and whether your assumptions are even remotely believable. If you define the wrong group, the analysis becomes mathematically tidy and scientifically dumb.
Blunt rule:
Pick the interference structure from subject-matter reality, not from whichever cluster variable happens to be easiest in the dataset.
Partial Interference: The Useful Simplification
One common compromise is partial interference. It assumes interference can happen within groups, but not across groups. Patients in the same ward may affect each other, but not patients in other wards. Households matter, neighborhoods do not. Villages matter, districts do not.
This assumption is strong, but it is often far more plausible than assuming no interference at all. It also gives you a workable framework for cluster-randomized trials and grouped observational studies.
Why partial interference matters:
It lets you define causal effects as a function of group-level treatment coverage, such as the effect on an untreated patient when 70 percent of their ward is treated.
Exposure Mapping: Stop Treating Spillover as Binary
Most interference settings are not just “someone else got treated” versus “nobody else got treated.” What matters may be the proportion treated, the number of treated contacts, the treatment status of a key physician, or the density of treated neighbors within a network radius.
That is why analysts often define an exposure mapping: a rule that converts the treatment pattern around a unit into a meaningful exposure summary. Examples include:
- proportion of vaccinated classmates,
- share of ICU beds under a staffing model,
- number of treated household members,
- presence of any treated close contact,
- network-weighted treatment coverage.
This is where design thinking matters more than math. A terrible exposure mapping can make a sophisticated analysis useless.
A Clinical Example: Antibiotic Stewardship in Hospital Wards
Suppose a stewardship program is rolled out to selected prescribers inside a hospital. You want to know whether it reduces broad-spectrum antibiotic use and downstream resistant infections. The interference problem is immediate. One physician's prescribing changes team norms, pharmacy behavior, microbiology feedback, and the microbial environment other patients experience.
A patient managed by an untreated clinician can still benefit if the ward around them changes. That means the patient-level contrast “program vs no program” is incomplete. You may care about:
- the effect of being directly exposed to a trained prescriber,
- the spillover effect of ward-level program coverage, and
- the overall effect of implementing stewardship across the whole ward.
Those are different questions, and a good study names which one it is trying to answer.
Why Standard Regression Usually Lies Here
If you fit an ordinary regression with one treatment indicator per person while ignoring group exposure, the coefficient usually mixes direct and spillover effects into something hard to interpret. Worse, if treatment assignment within groups is correlated with prognosis, behavior, or network position, you can get confounding on top of interference.
The common failure mode:
The model pretends units are independent, standard errors are too optimistic, and the treatment estimate silently absorbs exposure from treated neighbors.
That is not a small technical blemish. It changes the scientific meaning of the estimate.
Designs That Handle Interference Better
Cluster randomized trials
Randomizing at the group level often aligns better with real spillover structure and avoids contamination pretending to be noise.
Two-stage randomization
First randomize groups to treatment saturation levels, then randomize individuals within groups. This is one of the cleanest ways to separate direct and spillover effects.
Network-aware observational designs
When randomization is impossible, define network or cluster exposure carefully and adjust for covariates at both unit and group levels.
Policy saturation analyses
Sometimes the real estimand is not individual treatment at all, but the effect of increasing coverage from, say, 20 percent to 80 percent.
The Assumptions You Still Need
Interference changes the setup, but it does not suspend causal discipline. You still need versions of exchangeability, positivity, and consistency. They just become more complicated because treatment is now partly an individual exposure and partly an environmental one.
| Assumption | What it means here | How it fails |
|---|---|---|
| Exchangeability | Given measured covariates, treatment and exposure to treated others are as-if random | Network position, clinician selection, or ward severity drives both exposure and outcome |
| Positivity | You observe enough variation in both individual treatment and group treatment coverage | Some groups are always fully treated or never treated |
| Consistency | The defined exposure strategy corresponds to a meaningful intervention | “70 percent treated” can happen through many qualitatively different mechanisms |
What Researchers Usually Get Wrong
- They mention contamination only as a limitation instead of redesigning the estimand.
- They randomize individuals in tightly connected settings, then act surprised when effects dilute.
- They ignore network or cluster structure in both the analysis and the standard errors.
- They report an average treatment effect without defining treatment coverage around each unit.
- They talk about herd effects, peer effects, or contamination interchangeably as if those are the same question.
My take is harsh here because it needs to be: once spillover is plausible, vague language becomes methodological camouflage.
How to Report Interference Honestly
Reviewers should expect clear answers to the following:
- What units can interfere with each other?
- How was neighborhood, cluster, or network exposure defined?
- What causal effect is being estimated: direct, indirect, total, or overall?
- Was the design aligned with the interference structure?
- How much support exists for different treatment coverage levels?
- Were sensitivity analyses done for alternative exposure mappings or cluster definitions?
Reporting rule:
Never call a result “the treatment effect” in an interference setting unless you define whose treatment and whose surrounding exposure you changed.
When Simpler Thinking Is Still Fine
Not every study needs full network causal machinery. Sometimes the right move is simply to randomize by cluster, analyze at the cluster level, and admit the effect is policy-level rather than individual-level. That is often better than forcing a fake individual estimand onto a social process.
Complexity is not virtue. Credible alignment between question, design, and analysis is virtue.
The Bottom Line
Interference is not an exotic edge case. In a lot of clinical, behavioral, and policy research, it is the default reality. Treatments spill. People affect each other. Systems react. If your causal framework ignores that, you are not simplifying the world. You are describing the wrong world.
The fix is not to panic and build an unreadable network model for every project. The fix is to define the group where spillover matters, choose an estimand that matches that reality, and design the study so the resulting effect has a clean interpretation.
My opinionated summary is simple: when treatment can spread through contact, workflow, or environment, the honest question is rarely “what happens if this person is treated?” It is “what happens when treatment changes the local system around them?” That is the question worth estimating.
Keep reading
Don't stop at one method.
Good methods judgment comes from contrast. Read the neighboring guides, see where the assumptions diverge, and avoid treating every observational problem like it needs the same hammer.
Causal Readiness: When a Huge Linked Dataset Still Cannot Identify an Effect
A practical guide to causal readiness in linked health and administrative data. Learn why scale and propensity-score overlap are not enough when treatment, need, comparators, or outcomes are poorly measured.
Triangulation in Clinical Research: When One Elegant Design Still Leaves the Same Blind Spot
A practical guide to triangulation in clinical research. Covers what counts as genuinely complementary evidence, how to map designs to specific threats, and what reviewers should demand before trusting “robustness” claims.
Prevalent-User Bias: When Your Drug Study Starts After the Interesting Harm Already Happened
A practical guide to prevalent-user bias for clinical researchers. Covers depletion of susceptibles, survivor selection, post-treatment baseline covariates, and what reviewers should demand before trusting late-entry treatment cohorts.