Competing Risks: When Kaplan-Meier Tells the Wrong Clinical Story
A lot of clinical papers ask a sensible question in a bad statistical language. They want to know the risk of an event, but some patients experience another event first that makes the original one impossible. Death before stroke. Transplant before dialysis initiation. Discharge before in-hospital infection. That is a competing risk problem.
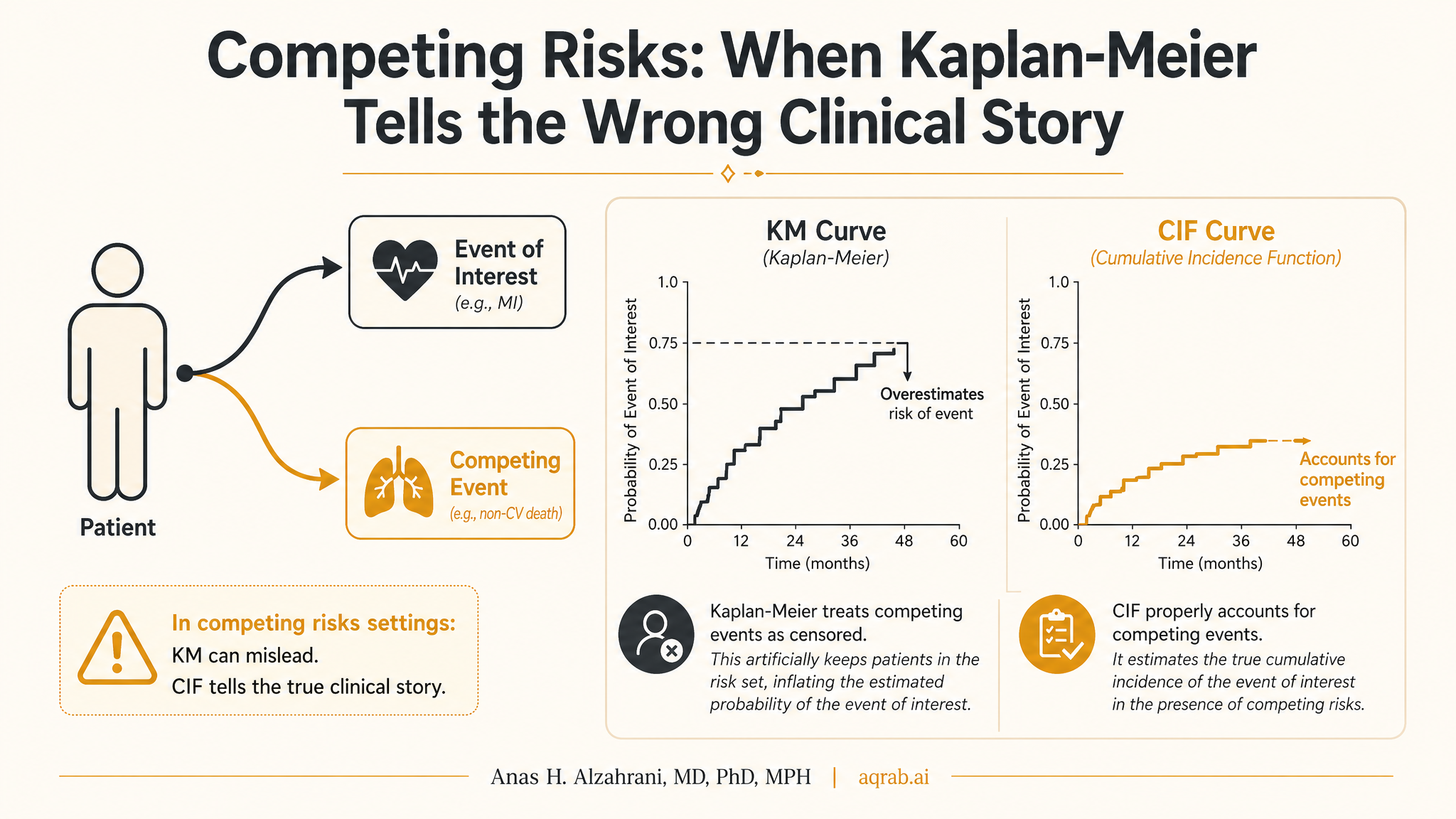
My take is blunt: if a competing event blocks the outcome, standard Kaplan-Meier curves can tell a clinically misleading story. They treat patients with competing events as if they were merely censored and still somehow available to fail later. They are not. Once the competing event happens, that outcome path is gone.
What a Competing Risk Actually Is
A competing risk is an event that either prevents the event of interest from occurring or fundamentally changes its meaning. In many medical studies, the classic competing event is death. If the outcome is nursing-home placement, readmission, amputation, or cancer recurrence, death can happen first and shut the door on that future event.
Core problem:
Standard survival methods assume censored patients could still experience the event later. Patients with a true competing event usually cannot.
That is why treating competing events as ordinary censoring can inflate the apparent event probability and distort the interpretation of treatment effects.
The Fast Intuition
Imagine you are studying 1-year risk of major amputation in patients with severe limb ischemia. Some patients die early. If you censor them in a Kaplan-Meier analysis, the method acts as if they simply disappeared from observation while remaining statistically eligible for amputation later. That fiction pushes the estimated amputation probability upward.
Clinically, that is nonsense. A dead patient is not a patient still at risk for future amputation in the same disease trajectory. The wrong method answers the wrong question with false confidence.
Where This Shows Up Constantly
Cardiovascular studies
Nonfatal MI, stroke, bleeding, and revascularization are often pre-empted by death.
Cancer outcomes
Recurrence, second-line treatment, or progression can be blocked by death from cancer or other causes.
Hospital epidemiology
In-hospital infection, ICU transfer, or deterioration can be cut off by discharge or death.
Kaplan-Meier vs Cumulative Incidence: Not the Same Job
| Method | What it estimates | Main weakness in competing-risk settings |
|---|---|---|
| Kaplan-Meier | Event probability under censoring assumptions | Treats competing events like noninformative censoring and can overestimate risk. |
| Cumulative incidence function | Observed probability of the event in the presence of competing events | Descriptive unless tied to a clear estimand and causal design. |
| Cause-specific hazard model | Instantaneous event rate among those still event-free | Hazard ratios are easy to misread as direct statements about cumulative risk. |
| Fine-Gray subdistribution model | Association with the cumulative incidence function | Interpretation is less intuitive and often abused as if it were a standard hazard model. |
The key point is simple: risk and hazard are not interchangeable, and competing risks make that difference impossible to ignore.
The Clinical Example
Suppose you compare two anticoagulation strategies after valve surgery and your outcome is ischemic stroke within one year. Treatment A reduces stroke but increases fatal bleeding. Treatment B causes fewer fatal bleeds but more nonfatal strokes.
- If you model stroke with Kaplan-Meier and censor deaths, you can exaggerate stroke probability.
- If you use a cause-specific hazard model, you learn how treatment changes the instantaneous stroke rate among patients still alive and stroke-free.
- If you use the cumulative incidence function, you learn the real-world probability of stroke while acknowledging that death can happen first.
Those are not competing statistical brands. They are answers to different questions. The analysis should follow the clinical decision, not the analyst's habit.
Cause-Specific Hazard or Fine-Gray?
This is where people get weirdly tribal. The correct answer is not “always Fine-Gray” or “always cause-specific.” It depends on the estimand.
Use cause-specific hazards when...
you care about etiologic questions, biological mechanisms, or how treatment changes the rate of the event among patients still at risk.
Use Fine-Gray when...
you care about prognosis or absolute event burden in the real world, where competing events remain part of the observed clinical path.
Even then, be careful. A subdistribution hazard ratio is not a clean instantaneous risk ratio. It is a modeling device tied to cumulative incidence. If you cannot explain it in plain language, do not pretend the reader can.
Why This Matters for Causal Inference
Competing risks are not just a survival-analysis technicality. They force you to define what effect you actually want. Are you asking about total treatment effect on an outcome in a world where treatment also changes mortality? Or the direct pathway to the nonfatal outcome if death were somehow eliminated? Those are different causal questions.
This is why sloppy censoring can quietly turn a causal question into a mathematically convenient but clinically meaningless one.
Common Mistakes
1. Reporting Kaplan-Meier incidence with death as censoring
That usually overstates event risk when death truly competes with the outcome.
2. Treating Fine-Gray and cause-specific models as interchangeable
They target different quantities. Same dataset, different question.
3. Forgetting that discharge can be a competing event too
Hospital studies love to ignore this and then overstate nosocomial risk.
4. Interpreting hazard ratios like cumulative risks
Hazard ratios say nothing directly about absolute incidence without additional structure.
What Good Papers Report
- The event of interest and every clinically meaningful competing event.
- Why each competing event is competing rather than just censoring.
- The estimand: etiologic rate effect, prognostic cumulative risk, or something else.
- Cumulative incidence curves when the question is about observed event probability.
- Cause-specific and/or Fine-Gray models with interpretation matched to the estimand.
- Plain-language explanation of what the effect estimate means clinically.
Reviewer Red Flags
- “Kaplan-Meier incidence” for a nonfatal outcome when death is common.
- No mention of competing events despite obvious mortality or discharge pathways.
- Fine-Gray used automatically with no stated clinical question.
- Hazard ratios interpreted as direct differences in patient-level probability.
- No cumulative incidence plot for outcomes where absolute burden is the real decision target.
The Practical Bottom Line
Competing risks force methodological honesty. If another event can happen first and shut down the outcome you care about, you cannot analyze the data as if that pathway did not exist. Kaplan-Meier is not “conservative.” In these settings it is often wrong for the clinical question people think they are answering.
The fix is not more software gymnastics. It is choosing the estimand first. If you want real-world event probability, use cumulative incidence thinking. If you want etiologic rate comparisons, use cause-specific hazards and say so. But stop censoring competing events out of the story and calling the result clinical truth.
Keep reading
Don't stop at one method.
Good methods judgment comes from contrast. Read the neighboring guides, see where the assumptions diverge, and avoid treating every observational problem like it needs the same hammer.
Restricted Mean Survival Time: When Hazard Ratios Are Not the Clinical Answer
A practical guide to restricted mean survival time for clinical researchers. Covers what RMST estimates, when it beats the hazard ratio, how to choose the time horizon, and how to report results clinicians can actually interpret.
Landmark Analysis: Useful, Honest, and Frequently Overclaimed
A practical guide to landmark analysis for clinical researchers. Covers delayed treatment, immortal time bias, conditional survivor populations, landmark selection, and why a cleaner timeline still changes the causal question.
Informative Censoring: When Dropout Is Part of the Bias
A practical guide to informative censoring for clinical researchers. Covers loss to follow-up, treatment discontinuation, database exit, inverse probability of censoring weights, and why dropout can bias survival and causal estimates when it depends on prognosis.