Immortal Time Bias: The Fake Survival Advantage Hiding in Bad Study Design
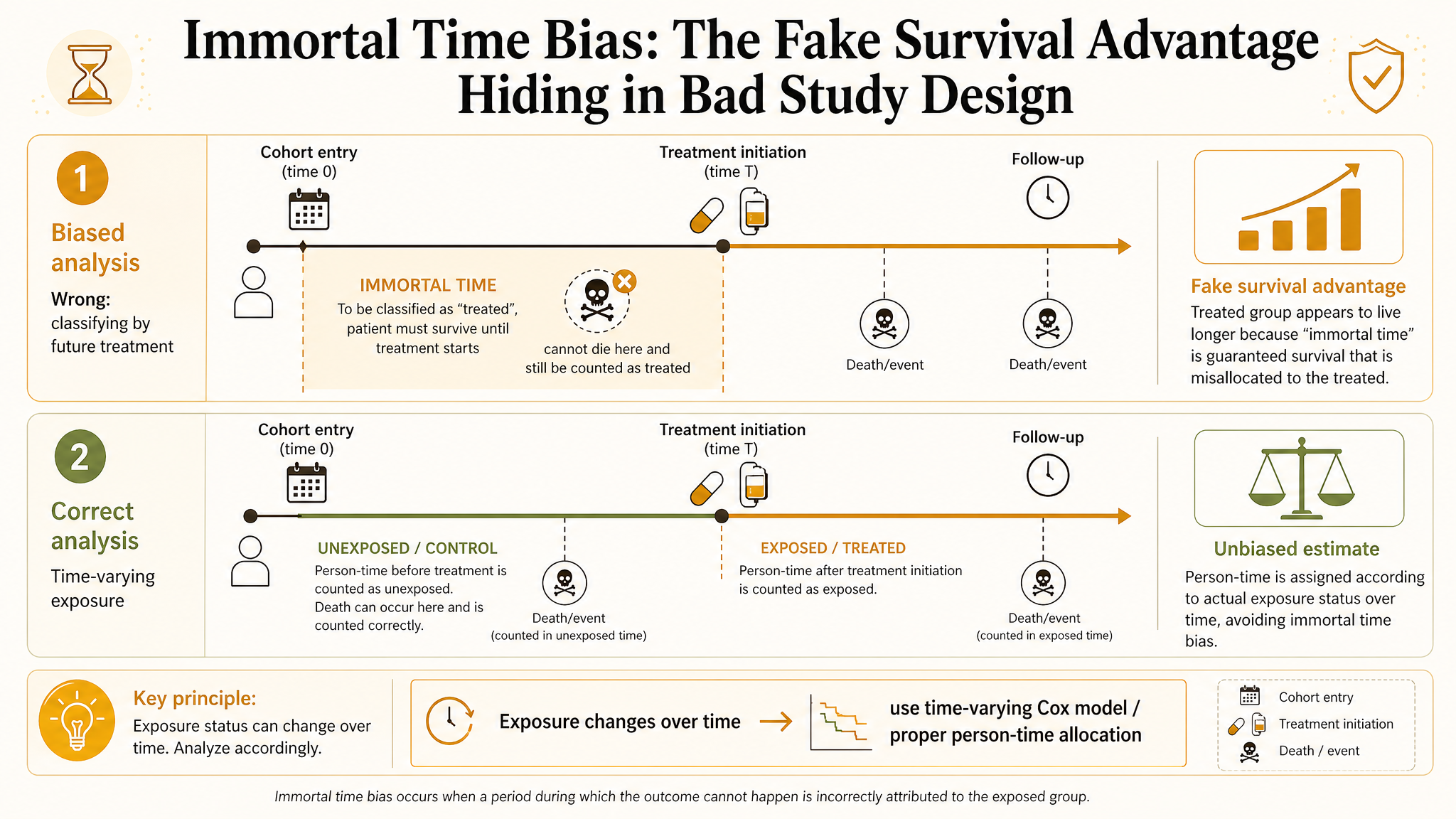
Immortal time bias is one of the dumbest ways to manufacture a treatment benefit, and it keeps showing up in serious journals. The trick is simple: classify patients by something that happens after cohort entry, then give the treated group credit for survival time they had to accumulate in order to even qualify as treated. That period is called immortal because the patient had to stay alive, event-free, and under observation long enough to reach treatment classification.
My take is blunt. If eligibility, treatment assignment, and follow-up do not start on a coherent timeline, your hazard ratio is not a causal estimate. It is bookkeeping fraud wearing a Cox model. Most immortal time bias is not subtle statistics. It is bad design, bad time alignment, and people acting like time starts whenever the analysis becomes convenient.
What Immortal Time Bias Actually Is
Immortal time bias happens when part of follow-up is incorrectly assigned to the exposed group even though the patient had not yet received the exposure. To be labeled exposed, the patient must survive that waiting period. That automatically makes the exposed group look healthier, even if the treatment does nothing.
Core problem:
You counted survival time before treatment as if it were survival because of treatment.
Once you see it, you cannot unsee it. The bias is not magical. It is created by giving one group guaranteed survival time that the other group never gets.
The Classic Bad Example
Imagine a cohort of patients hospitalized with heart failure. You define the treatment group as patients who received a specialist consultation within 30 days of admission. Everyone else is untreated. Then you start follow-up at admission and compare mortality.
- Patients who died on day 3 can never enter the consultation group.
- Patients classified as treated had to survive until the consult happened.
- That pre-consult time is now incorrectly helping the treated group look safer.
Congratulations, you have built a fake treatment benefit out of the calendar.
Why the Bias Can Be Huge
Immortal time bias is not a small technical nuisance. It can reverse the direction of an effect. In pharmacoepidemiology and comparative effectiveness work, this bias has made useless or harmful treatments look protective simply because treated patients had to live long enough to receive them.
What gets inflated
Apparent survival in the treated group, especially when treatment is initiated after discharge, after stabilization, or after multiple eligibility steps.
What gets hidden
Early deaths, treatment delays, contraindication patterns, and the fact that sicker patients may never make it into the so-called exposed cohort.
How to Spot It Fast
If I am screening a paper for immortal time bias, I ask three questions immediately:
When does follow-up start?
If follow-up starts before treatment assignment can logically occur, I get suspicious fast.
When is exposure defined?
If exposure is based on future information like “received drug within 90 days,” there is danger.
Could someone die before qualifying as treated?
If yes, the design needs explicit handling of that waiting time. Otherwise the treated arm is getting free survival credit.
Where Researchers Commonly Create It
- Defining exposure as filling a prescription within a window after diagnosis or discharge.
- Comparing organ transplant recipients with non-recipients from the time of waitlist entry.
- Calling patients “adherent” based on future follow-up behavior, then analyzing survival from baseline.
- Assigning ICU interventions based on treatments received later during the admission.
- Using responder analyses where “response” requires surviving long enough to be assessed.
Notice the pattern. The label comes from the future, but the clock starts in the past.
Immortal Time Bias vs Time-Varying Treatment
The real issue is not that treatment starts later. Delayed treatment initiation is normal in real data. The issue is pretending that a time-varying treatment was a fixed baseline attribute. If treatment can begin during follow-up, your analysis has to respect that.
| Approach | What it does | Problem |
|---|---|---|
| Fixed exposed vs unexposed from baseline | Treats future treatment as if known at time zero | Classic immortal time bias |
| Time-varying exposure analysis | Keeps person-time unexposed until treatment actually starts | Still needs careful confounding control |
| Target trial emulation | Aligns eligibility, assignment, and follow-up explicitly | Requires design discipline most papers avoid |
Time Zero Is the Whole Game
Most immortal time bias collapses if you define time zero correctly. Time zero should be the moment when a person becomes eligible for the strategy comparison and could, in principle, enter either arm under the study design.
If those three are out of sync, the rest of the analysis is downstream damage control.
How to Fix It
There is no single universal fix, but the main solutions are straightforward.
Use time-varying exposure coding
Keep each patient unexposed until the actual treatment start date, then switch exposure status when treatment begins.
Redefine cohort entry
Start the clock at a treatment decision point where both strategies are genuinely possible, not at some earlier administrative event.
Emulate a target trial
Specify eligibility, assignment, grace periods, outcomes, censoring, and estimand before touching the data. This usually exposes the immortal time trap immediately.
Use clone-censor-weight when appropriate
For dynamic or grace-period strategies, clone-censor-weight approaches can align follow-up with strategy assignment without giving one arm impossible survival credit.
A Practical Clinical Example
Suppose you want to compare mortality for septic patients who received corticosteroids within 48 hours versus those who did not. If you define the steroid group based on receipt anytime in the first 48 hours, then start follow-up at ICU admission, anyone who dies before hour 36 can only land in the no-steroid group. That makes steroids look protective even before biology gets a vote.
A better design would explicitly compare strategies at ICU admission, allow a 48-hour grace period if justified, and handle treatment initiation during that period with design-aware methods rather than naive baseline labeling.
Why Matching Does Not Save You
People love to throw propensity score matching at everything, but matching does not fix immortal time bias if the exposure definition itself is future-based. You can balance a biased design perfectly and still get the wrong answer beautifully.
Important:
You cannot adjust your way out of a broken timeline. Alignment comes before modeling.
Reviewer Red Flags
- Exposure defined as treatment received within X days after baseline.
- Baseline characteristics measured at admission, but treatment classification requires future survival.
- Survival curves separate immediately even though treatment occurs later.
- No discussion of time zero, grace periods, or time-varying exposure.
- Claims of dramatic protective benefit from a delayed intervention in a very sick cohort.
If a paper has three of those, I assume the estimate is contaminated until proven otherwise.
What Good Reporting Looks Like
A serious paper should make the following explicit:
- the exact eligibility moment,
- the treatment assignment rule and whether treatment can start later,
- the definition of time zero,
- how person-time before treatment was handled,
- whether a grace period was allowed and why,
- how time-varying confounding was addressed if relevant,
- sensitivity analyses for alternative time alignment choices.
If the paper never tells you when the causal clock starts, it probably does not know.
The Bottom Line
Immortal time bias is not an advanced statistical curiosity. It is what happens when follow-up starts before treatment classification is logically fair. The resulting benefit can look dramatic, precise, and completely wrong.
The fix is not more complicated software. The fix is disciplined design: align eligibility, treatment strategy, and time zero like you actually mean the causal question. That is why target trial thinking matters so much. It forces you to respect time before time embarrasses you.
My blunt version: if patients had to survive to become treated, and you counted that survival as treatment benefit, the study did not discover efficacy. It discovered a calendar error.
Keep reading
Don't stop at one method.
Good methods judgment comes from contrast. Read the neighboring guides, see where the assumptions diverge, and avoid treating every observational problem like it needs the same hammer.
Causal Readiness: When a Huge Linked Dataset Still Cannot Identify an Effect
A practical guide to causal readiness in linked health and administrative data. Learn why scale and propensity-score overlap are not enough when treatment, need, comparators, or outcomes are poorly measured.
Triangulation in Clinical Research: When One Elegant Design Still Leaves the Same Blind Spot
A practical guide to triangulation in clinical research. Covers what counts as genuinely complementary evidence, how to map designs to specific threats, and what reviewers should demand before trusting “robustness” claims.
Prevalent-User Bias: When Your Drug Study Starts After the Interesting Harm Already Happened
A practical guide to prevalent-user bias for clinical researchers. Covers depletion of susceptibles, survivor selection, post-treatment baseline covariates, and what reviewers should demand before trusting late-entry treatment cohorts.