Misclassification Bias: When Your Variables Lie Before the Model Starts
A lot of researchers talk as if bias begins when the model is misspecified. Wrong. Bias often starts much earlier, the moment your dataset gives the wrong label to who was exposed, who had the outcome, or who even belonged in a covariate category. That failure has a name: misclassification bias.
My take is blunt: if your variables are sloppy, your causal estimate is built on fiction. People love to throw fancy adjustment at administrative codes, self-report fields, weak EHR phenotypes, and half-validated outcomes, then act shocked when the paper feels unstable. The model is not the first thing to audit. The labels are.
What Misclassification Bias Actually Is
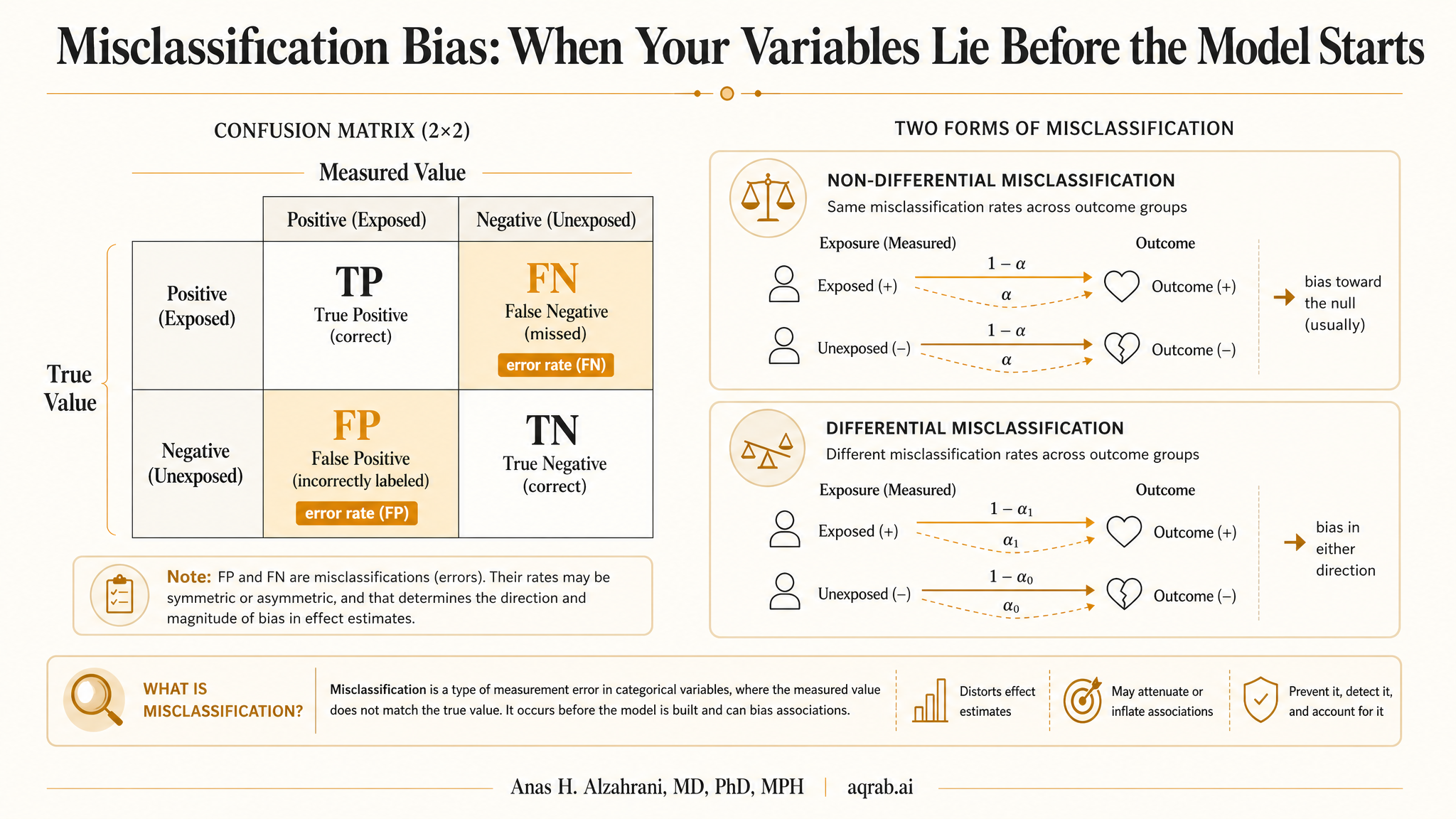
Misclassification happens when the observed value of a variable differs from its true value. A patient who really used a drug gets labeled unexposed. A true myocardial infarction gets missed. A smoker gets recorded as a nonsmoker. A covariate that should separate low from high severity gets measured with a dumb proxy.
Core problem:
When the labels in the data do not match reality, the effect estimate can be diluted, exaggerated, or even pushed in the wrong direction.
This can affect exposures, outcomes, confounders, and even eligibility criteria. The damage depends on what is misclassified, how often it happens, and whether the error differs across groups.
The Three Places It Usually Shows Up
Exposure
Prescription fill data, self-report, medication reconciliation, and procedure coding often disagree about who actually received what.
Outcome
Claims codes, screening practices, surveillance intensity, and adjudication quality change whether events are captured correctly.
Confounders
Smoking, frailty, disease severity, adherence, and socioeconomic status are often measured badly right where they matter most.
Differential vs Nondifferential Misclassification
This distinction matters because it changes the direction and size of the bias.
| Type | What it means | Why it matters |
|---|---|---|
| Nondifferential | Misclassification does not depend on the comparison group or the other variable | Often dilutes associations, but not always. That “biases toward the null” rule gets abused constantly. |
| Differential | Misclassification differs by exposure, outcome, or follow-up intensity | Can bias in any direction and can create dramatic fake findings. |
The lazy line that nondifferential misclassification always biases toward the null is only safe in a narrow set of simple binary situations. Once you are dealing with multiple categories, imperfect confounders, time-varying exposures, or outcome ascertainment tied to care intensity, that rule can fall apart fast.
The Fast Clinical Example
Imagine a study asking whether a new diabetes drug lowers heart failure admissions. Exposure is defined using prescription orders in the EHR rather than fills or actual initiation. Outcome is defined using hospitalization codes, but patients on the new drug are followed more closely and interact with cardiology more often.
- Some “exposed” patients never really started the drug.
- Some “unexposed” patients got the drug outside the captured network.
- Heart failure events are more likely to be detected in the intensively monitored group.
That is exposure misclassification plus outcome misclassification plus surveillance differences. The final hazard ratio is not just estimating treatment effect. It is also estimating how messy your data pipeline is.
Why Misclassified Confounders Are Especially Dangerous
Researchers spend a lot of time asking whether they included the right confounder and not enough time asking whether they measured it well enough to matter. A badly measured confounder can leave a huge amount of residual confounding behind while creating the illusion that the variable was “adjusted for.”
Severity is the classic problem. If disease severity drives treatment choice and outcome risk, but you only adjust for a crude baseline diagnosis code, you have not actually solved confounding by indication. You have rebranded it.
Common Sources of Misclassification in Real Studies
Administrative coding shortcuts
Claims and billing systems were built to get paid, not to make your causal design elegant. Codes can be incomplete, delayed, or strategically noisy.
Self-report
Smoking, alcohol use, medication adherence, diet, and sexual history are famous for recall problems and social desirability distortion.
Weak phenotyping
“One diagnosis code equals disease” is often absurd. Good phenotypes usually need algorithms, timing logic, repeat evidence, or chart review validation.
Time-window errors
Exposure and outcome labels often drift because the data window does not match the real clinical sequence. That is how classification mistakes become design mistakes.
Why Outcome Misclassification Can Be Differential Even When You Pretend It Is Not
If one treatment group gets more visits, more imaging, more lab checks, or more specialist attention, that group often gets more chances to have outcomes recorded. This is especially brutal for soft outcomes, early-stage diagnoses, adverse events, and complications that require active detection.
That means your observed outcome may partly reflect surveillance intensity rather than biology. The paper then acts as if event rates are comparable because the outcome definition was technically the same on both sides. Same code list, different detection process. Not the same thing.
The “Bias Toward the Null” Myth Needs to Die
People repeat this like a prayer: misclassification probably just attenuated the effect. Sometimes, yes. Often, no. Differential misclassification can inflate associations. Misclassified confounders can leave major bias untouched. Multilevel variables and thresholded measures can behave in messy nonlinear ways.
So when authors say, “any misclassification would likely bias results toward the null,” ask whether they actually demonstrated that. Usually they did not. Usually they are just trying to sound reassuring.
What Good Studies Do Instead
Validate key variables
Use chart review, registry linkage, adjudication, laboratory confirmation, or external gold standards when the variable drives the analysis.
Use richer phenotype definitions
Combine codes, timing, prescriptions, procedures, and repeated evidence rather than trusting a single lazy field.
Run quantitative bias analysis
Sensitivity analyses using plausible sensitivity and specificity values are far better than hand-wavy reassurance.
Be honest about detection processes
If outcome ascertainment differs by exposure, say it plainly and treat it as a core limitation, not a footnote.
Reviewer Red Flags
- Exposure defined by a single code or order field with no validation logic.
- Outcomes captured from administrative data but no sensitivity, specificity, or positive predictive value cited.
- Important confounders represented by crude proxies without any discussion of residual confounding.
- Claims that misclassification “likely biased toward the null” without a quantitative argument.
- Different follow-up intensity between groups, but no discussion of surveillance-driven event detection.
When you see those, do not let the confidence intervals distract you. Precision around the wrong label is still precision around the wrong label.
The Practical Bottom Line
Misclassification bias is not a technical side note. It is one of the main reasons causal estimates from real-world data drift away from reality. If your exposure is mislabeled, your outcomes are detected unevenly, or your confounders are weak proxies, the analysis is already under strain before modeling starts.
The fix is not glamorous: better phenotyping, better validation, better timing logic, and less pretending that routine EHR fields are automatically truth. If your variables lie, the model cannot save your dignity. Start by cleaning the labels.
Keep reading
Don't stop at one method.
Good methods judgment comes from contrast. Read the neighboring guides, see where the assumptions diverge, and avoid treating every observational problem like it needs the same hammer.
Measurement Error: When Bad Variables Break Good Causal Methods
A practical guide to measurement error for clinical researchers. Covers noisy exposures, weak confounder proxies, surveillance-driven outcomes, validation strategies, and why sophisticated causal methods cannot rescue bad variables.
M-Bias: When “Adjusted for Severity” Is Actually the Problem
A practical guide to M-bias for clinical researchers. Covers collider structures, severity-score traps, selected cohorts, and what reviewers should demand before trusting an adjusted estimate.
Bias Amplification: When Adjustment Makes Unmeasured Confounding Worse
A practical guide to bias amplification for clinical researchers. Covers near-instruments, noisy severity proxies, treatment-prediction traps, and why the wrong adjustment variable can magnify residual confounding instead of reducing it.