Overadjustment Bias: When More Covariates Make Causal Inference Worse
A depressing amount of observational research still treats covariate adjustment like a cleanliness ritual. Add age, sex, comorbidities, labs, severity scores, healthcare use, maybe a few biomarkers, then feel morally superior because the model is “fully adjusted.” That is not causal inference. That is just a big regression. Overadjustment bias happens when you condition on variables that should not be adjusted for, especially mediators, colliders, or post-treatment variables. Instead of reducing bias, you create it.
The core mistake is simple. Researchers memorize “adjust for confounders” and then quietly mutate it into “adjust for as many variables as possible.” Those are not the same idea. The right adjustment set is not the largest one. It is the one that blocks the right backdoor paths without opening new garbage paths.
The Core Principle
A variable belongs in your adjustment set only if conditioning on it helps identify the causal effect you care about. That usually means it is a pre-exposure common cause of treatment and outcome, or part of a valid design strategy justified by a causal graph.
Good causal adjustment asks one question:
Does this variable block a non-causal path between treatment and outcome without blocking part of the true treatment effect or opening a spurious path?
If the answer is no, leave it alone. More variables do not mean more rigor. They often just mean more opportunities to bias the estimate while sounding sophisticated.
The Three Usual Ways People Overadjust
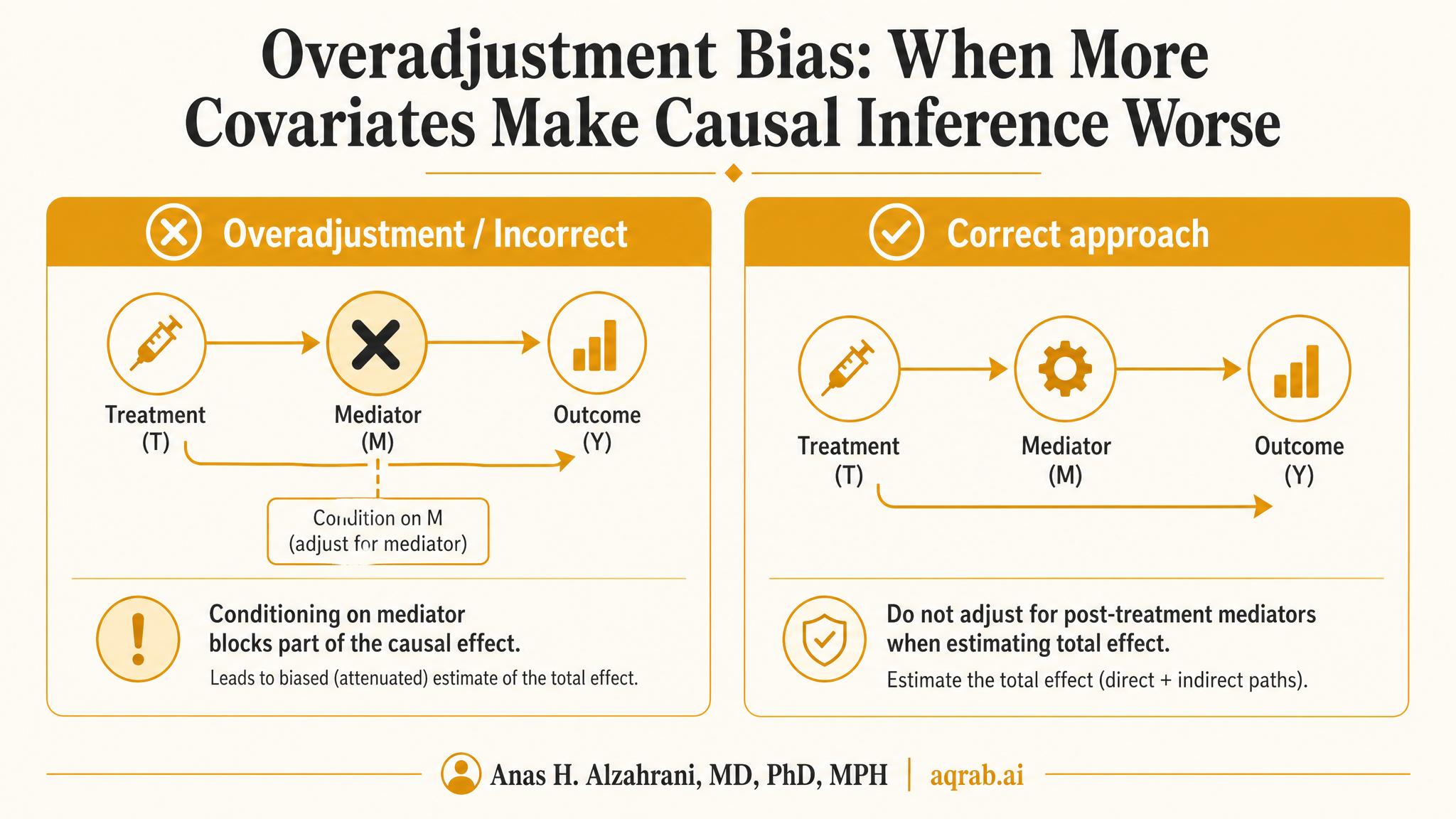
1. Adjusting for mediators
A mediator lies on the causal pathway from treatment to outcome. If you adjust for it while trying to estimate the total effect, you block part of the very effect you wanted to measure.
2. Adjusting for colliders
A collider is caused by two variables. Conditioning on it opens a path that was previously blocked. That means you can manufacture an association that did not exist before adjustment.
3. Adjusting for post-treatment variables
Once a variable is affected by treatment, it becomes dangerous. It may be a mediator, a collider, or part of treatment-confounder feedback. Either way, naive adjustment is usually wrong.
Why Mediator Adjustment Breaks the Total Effect
Suppose you want the effect of an antihypertensive drug on stroke. Blood pressure reduction sits on the pathway. If you adjust for achieved blood pressure after treatment initiation, you are no longer estimating the total effect of treatment on stroke. You are estimating something closer to a controlled direct effect, and usually a badly defined one at that.
Hard truth:
“We adjusted for intermediate response markers to isolate the independent effect” is often just a fancy way of saying “we adjusted away part of the treatment effect and called the remainder causal.”
That move is only defensible if the estimand is explicitly a direct effect, the assumptions are stated, and treatment-induced confounding is handled appropriately. In most papers, none of that happens.
Collider Bias Is Even Nastier
Collider bias feels counterintuitive because the bad thing happens after you adjust. Imagine treatment affects clinic follow-up, and baseline severity also affects clinic follow-up. If you restrict the analysis to patients with follow-up visits, or adjust for a follow-up-dependent variable, you may open a path between treatment and severity through that shared consequence.
Classic collider logic:
- Treatment → follow-up intensity
- Severity → follow-up intensity
- Condition on follow-up intensity
- You just created a non-causal link between treatment and severity
This is why “complete case” analyses, registry-only subsets, and EHR studies conditioned on utilization are often causally filthy even when the regression output looks polished.
A Clinical Example That Fails Fast
Imagine you are studying whether early ICU transfer reduces mortality in sepsis. A team decides to adjust for vasopressor use measured after ICU transfer because it is a marker of severity. That is a mess. Vasopressor use may be affected by transfer timing, clinician behavior, and evolving patient status. It is not a clean baseline confounder. It is a post-treatment variable sitting in the middle of the story.
Once you adjust for it, you risk stripping away part of the pathway through which early ICU care changes outcomes, while also introducing bias through treatment-induced selection mechanisms. The estimate becomes harder to interpret, not more credible.
The DAG View
Overadjustment becomes obvious once you draw the graph. DAGs force you to ask what comes first, what causes what, and whether a variable is a confounder, mediator, collider, or descendant of one of those. Without a DAG, people routinely mistake central-looking variables for confounders just because they sound clinically important.
Adjust
Pre-exposure common causes of treatment and outcome, if they are needed to block backdoor paths.
Do not naively adjust
Mediators, colliders, descendants of colliders, and variables measured after treatment without a clear causal justification.
Why “Baseline Severity” Is Often Used Sloppily
Researchers love severity variables, and sometimes rightly so. Baseline severity often is a confounder. The problem is that many datasets measure “severity” after treatment starts, after diagnosis, after admission, or after clinician contact patterns have already been shaped by the exposure.
At that point, the variable is no longer clean baseline severity. It is a mixed object contaminated by treatment, surveillance, and evolving disease course. Calling it a confounder does not make it one.
Overadjustment in Propensity Score Models
This problem is not limited to regression. People dump post-treatment labs, utilization markers, and outcome-adjacent variables into propensity score models, then congratulate themselves for excellent balance. Balance on the wrong variables is not a win. It is evidence that you built the wrong design very efficiently.
A propensity score should summarize treatment assignment based on pre-treatment covariates. Once you start feeding it variables affected by treatment or downstream of unmeasured processes, you are no longer modeling treatment assignment. You are laundering bias through a score.
Common Red Flags in Published Papers
“Fully adjusted model” with no DAG
If the paper cannot explain why each covariate belongs in the set, “fully adjusted” means almost nothing.
Adjustment for biomarkers after exposure starts
These are usually mediators or post-treatment proxies, not innocent confounders.
Restriction to observed users, attenders, or survivors
That often conditions on colliders created by care-seeking or survival processes.
Sensitivity analysis defined as “add more covariates”
If those extra covariates are causally wrong, the sensitivity analysis just measures how robust the mistake is.
What To Do Instead
Start with the estimand. Are you estimating a total effect, a direct effect, or something else? Then draw the DAG before writing the model formula. Classify each candidate covariate by time order and causal role. If you do not know whether a variable is pre-treatment or downstream of the exposure, that is not a nuisance detail. That is the analysis.
- Define the causal question first.
- Separate pre-treatment variables from post-treatment variables ruthlessly.
- Use DAGs to identify a minimally sufficient adjustment set.
- Do not chase predictive performance at the expense of causal validity.
- If you truly need mediator or time-varying pathway analysis, use methods built for that job.
When Adjustment for an Intermediate Can Be Legitimate
There are times when you intentionally model pathways through intermediates, but that is a different problem. Mediation analysis, interventional direct and indirect effects, marginal structural models, and g-methods exist because naive adjustment is not enough. If your question is mechanistic, switch methods. Do not pretend ordinary regression plus a few intermediates solved it.
What Reviewers Should Expect
- A clear estimand, total effect versus direct effect.
- A DAG or equivalent causal justification for the adjustment set.
- Explicit timing of every adjusted variable relative to treatment initiation.
- An explanation for any post-treatment variable included in the model.
- Language that distinguishes prediction from causal identification.
Bottom Line
Overadjustment bias is what happens when statistical ambition outruns causal thinking. The model looks richer, the table gets longer, and the estimate gets worse. Adjusting for more variables is not a badge of rigor. It is only rigorous when the variables belong there.
If a variable sits downstream of treatment, sits at the intersection of two causes, or sits on the causal pathway you want to estimate, touching it casually can break the study. Draw the graph first. Then earn the regression.
Keep reading
Don't stop at one method.
Good methods judgment comes from contrast. Read the neighboring guides, see where the assumptions diverge, and avoid treating every observational problem like it needs the same hammer.
M-Bias: When “Adjusted for Severity” Is Actually the Problem
A practical guide to M-bias for clinical researchers. Covers collider structures, severity-score traps, selected cohorts, and what reviewers should demand before trusting an adjusted estimate.
Measurement Error: When Bad Variables Break Good Causal Methods
A practical guide to measurement error for clinical researchers. Covers noisy exposures, weak confounder proxies, surveillance-driven outcomes, validation strategies, and why sophisticated causal methods cannot rescue bad variables.
Bias Amplification: When Adjustment Makes Unmeasured Confounding Worse
A practical guide to bias amplification for clinical researchers. Covers near-instruments, noisy severity proxies, treatment-prediction traps, and why the wrong adjustment variable can magnify residual confounding instead of reducing it.